The typologies of both Jung and Kretschmer are rooted in their psychiatric work. Jung, for example, in his 1913 paper that announced his interest in types identifies the schizophrenic as an introvert, albeit a regressed introvert, and the hysteric as a regressed extravert. Kretschmer, in his turn, described the manic depressive as a pyknic, and his schizophrenics as predominately asthenic or leptosomatic. And their work helped establish a psychiatric common ground, which has been tested many times, and in which the schizophrenic is introverted and ectomorphic, and the manic-depressive extraverted and endomorphic and mesomorphic. But despite the strong psychiatric origins of Jung's typology it would probably be fair to say that the application of his typology to psychopathology has been neglected, with some notable exceptions.
J.H. van der Hoop, who attempted to blend both Jungian and Freudian interpretations in his book on psychological types, Conscious Orientation (1937), makes some remarks on the relationship between Jung's types and Kretschmer's descriptions. The obvious starting place is a comparison of introverts and extraverts with schizothymes and cyclothymes, but he goes further and makes some other interesting suggestions. For example, "we should most likely expect to find severe manic-depressive states developing in extraverted instinctives (sensation types) and in extraverted intuitives." (p. 227) He notes in Kretschmer's descriptions of the manic-depressive both their materialistic disposition with their enjoyment of the good things of life which leads him to the conclusion that they are extraverted sensation types, and he interprets their wealth of ideas and an eye for opportunity as an indication of the presence of extraverted intuition types. Then he makes an interesting connection between the introverted intuitive type and Kretschmer's schizoids. "From a clinical point of view, the strongly introverted intuitive seems to offer the closest comparison with the manifestations of schizophrenia, and when there are strong influences derived from complexes in persons of this type, they sometimes resemble very closely Kretschmer's schizoids." (p. 246)
Let's look more closely at van der Hoop's suggestion that the manic-depressives are both extraverted sensation types and extraverted intuition types. He refers to Kretschmer's descriptions which point of their enjoyment of life, their zestful eating and drinking, and so forth, as signs of their extraverted sensation, whereas their wealth of ideas, daring and overestimation of the self seem to indicate the extraverted intuition type. We can pursue this matter a little further by looking at the portrait that Kretschmer paints of Quick, the cheery hypomanic type. Quick is 40 years old and with him no one can get in a word edgewise. He wanders from the subject and comes back again, and as "he is closing the door there are always one or two things that occur to him and which he must quickly get off his chest." (p. 141) Van der Hoop's estimation that this is an extraverted sensation type is supported by comments like this: "With one glance round he has taken in all the decoration of a room, down to a small nail up on the ceiling, and has figured out the price of every object." (P. 141-2) He has a knack for making money. He came under Kretschmer's care for his increasingly outrageous conduct which culminated in having a brass band celebrate the birthday of his mother-in-law starting a 6 o'clock in the morning. When he was hospitalized he Soon knew the regime of the whole hospital and filled his room with knickknacks, including a toilet paper dispenser, which, whenever a piece of paper was torn off, gave forth with "Make Hay While the Sun Shines". He is consistently and solidly people-oriented and wins their tolerance even for his outrageous conduct, all of which are not traits of the extraverted intuiter. He simulates the extraverted intuiter in terms of his constant flow of ideas, but these ideas are very concrete and executed with a sureness of worldly touch that is often lacking in the extraverted intuiter.
K.W. Bash (1961), while not relating the specific psychological type to the various kinds of psychopathology, does examine the psychological function in relation to psychiatric illnesses. Delusion and illusion, for example, are related to the function of intuition.
Bisbee, Mullaly and Osmond (1982) gave the MBTI to 372 psychiatric patients close to the time of their admission and found that schizophrenic patients tended to be more introverted with the introverted sensation thinking type, the introverted sensation feeling type and the introverted feeling sensation type predominating, while the manic-depressives were more extraverted with the extraverted feeling sensation type, the extraverted intuition thinking type and the introverted feeling intuition type over represented. Part of the paucity of the studies in this area can be attributed to the diagnostic problem which returns with a vengeance when it is a case of people with serious psychiatric illnesses. Jung made it clear that the schizophrenic who shows an introverted character during the incubation of his illness can reach a stage of morbid compensation where "he seems constrained to draw attention to himself by his extravagant, insupportable, or directly aggressive behavior." (1913) He could then easily be typed at variance to his natural disposition.
This difficulty of typological diagnosis makes it hard to assess studies on the pre-morbid characteristics of schizophrenic children. Type is often difficult to discern in the fluid and unformed personalities of the children, and this problem is compounded by the possibility that the sub-clinical onset of schizophrenia may express itself, as Jung stated, in an acting out coming from the other side of the personality. Thus, shy, withdrawn children might be found rarely to become schizophrenic, while unsocialized aggression could be a prominent characteristic without either finding necessarily contradicting the affinity for schizophrenia to express itself in the introverted personalities.
But the difficulty encountered in trying to estimate type is far outweighed by the potential benefits. Just who is the person who is ill? What were they like before their illness, if there was ever a time before? And to what kind of personality are they meant to return? There is a certain ambiguity in psychiatric terminology when we fail to distinguish between the description of normal differences and their exaggeration in the diseased process. What are we to make out of a description of the schizoid personality described by Seymour Kety as follows:
"He is withdrawn, he has few friends, he is very strongly religious and he reads a great deal of philosophy which is something schizophrenics often do. He has an inappropriate grin when he talks. He flunked out of school, although he is obviously intelligent. He never married. He doesn't go out often and his room is very messy. He looks unkempt. He has a lower level job than his social class or intelligence would warrant." (Rosenthal, The Transmission of Schizophrenia, p. 73)
Are we seeing society's view of the introvert or some mild phase of schizophrenia? We will not find the answer until we can subtract normalcy from the equation. But how can we make this subtraction when it is so difficult to diagnose psychological types? The answer lies in our project of creating an integrated typology that would consider not only psychological type but somatotype and eventually a biochemical typology as well.
What can help us in this endeavor is the important psychiatric work that Sheldon did to reformulate the basic three psychiatric categories which stemmed from Kraepelin, and relate them to his work in somatotypes and temperament.
In 1949 with the publication of his Varieties of Delinquent Youth Sheldon was like a prophet peering in the mists trying to catch a glimpse of a biologically founded criminology and psychiatry. Sheldon thought that what the psychoanalyst called the unconscious just might be the body itself, and the body "is really an objectification, a tangible record, of the most long-standing and most deeply established habits that have been laid down during a long succession of generations." (p. 4) And so he started with an objective record of the body with his somatotype photos. And when he studied the young men at the Inn he saw what he called the asthenic and burgeoned estates. Asthenia was a failure to flower, a retreat of the organism from its proper line of development, while burgeoning was an overexuberance, an overaccumulation of mass that becomes a debilitating burden. And what is true at the level of somatotype Sheldon felt would be seen at the cellular level, as well. When he writes, "A cell is a living thing with a personality. Whatever the asthenic estate is at bottom and the burgeoned estate, these are without doubt expressions of the personality of the cells of the individual..." (p. 800), he is trying to read behind and through the somatotype and divine the biological foundations of personality and behavior that we are only beginning to unravel today.
Even the uneven development or dysplasias he found in the somatotype he felt could be found at the cellular level, as well. When he came across individuals who had mesomorphic skin and hair in some parts of their bodies, and ectomorphic skin and hair in others, he reasoned, because of the connection between skin and the nervous system, that "it is not improbable that similar dysplastic variations in nervous and brain structure exist..." (p. 808)
How more comfortable would he have felt if instead of being confronted with a thoroughly environmental view of crime he could have drawn on the modern studies such as the following:
William Walsh compared the trace elements in the hair of 24 matched pairs of violent and non-violent siblings, and 96 extremely violent men, and 96 controls. The violent people showed increased levels of lead, cadmium and calcium, and excessively low levels of lithium, zinc and cobalt. Even the violent could be broken down into two classes: those subject to sudden fits of rage, and those who are anti-social, and these groups could be distinguished by the trace elements in their hair. The impulsively violent men showed high levels of sodium and low levels of copper, while the anti-social men showed high levels of copper and low levels of sodium. Walsh also felt that the trace element profiles of the hair of normal people tended to divide them into six types.
Michael McGuire found that the dominant males in 45 different monkey colonies had twice as much serotonin in their blood as the other males, and the serotonin fluctuated according to their social status. When a monkey was acknowledged as the leader, his serotonin level rose. When he was deposed, it fell. There has also been some evidence of high serotonin levels in human leaders and Type A personalities. Paradoxically, low levels of serotonin have shown up in violent people, and has been detected by means of their 5-HIAA levels, which is a result of serotonin breakdown. In a study of 38 violent servicemen Gerald Brown and Frederick Goodwin discovered that the level of serotonin matched the level of violence. The lower the serotonin level the higher the violence. There is also a connection between low -HIAA and suicide. Markku Linnoila and Matti Virkunen compared the 5-HIAA levels of psychopaths who had committed apparently senseless and random murders and what they called paranoid murderers who had acted with premeditation, and found that the psychopaths had lower 5-HIAA levels. Mass murderers have also been found to have unusually low levels of 5-HIAA. (cf. Hooper and Teresi)
Serotonin has been connected with inhibition and we are probably looking at something similar to asthenia that Sheldon had begun to discern at the level of somatotype. It is inevitable that these discoveries would pose the question of biochemical treatment of violence, and one aspect is the orthomolecular treatment of delinquent and criminal behavior. If there is a possibility to alter behavior by chemical means, the safest way to do this would be to do it by changing the proportions of the natural substances that already exist in our diet. Even when prisons offer a halfway decent diet, the prisons eat selectively or reject meals entirely in favor of junk food.
In Ecologic-Biochemical Approaches to Treatment of Delinquents and Criminals we have a collection of articles that are beginning to spell out an orthomolecular approach to the very problems Sheldon confronted in his 200 young men, but without the tools to make a biological attack on their difficulties. He would have been happy to read Allan Cott's "The Etiology of Learning Disabilities, Drug Abuse and Juvenile Delinquency" or William Philpott's "Ecological Aspects of Antisocial Behavior".
Sheldon's earlier autopsy work which was instrumental in his describing the basic components of somatotype in terms of the various embryonic layers had been augmented by the work of Nolan D.C. Lewis. Lewis "in a series of more than 2,000 autopsies of psychotic patients had shown that whenever the diagnosis hebephrenic dementia praecox (schizophrenia) occurred, vascular hypoplasia, especially in the terminal vessels, was a constant finding". ("Psychotic Patterns and Physical Constitution", p. 840) And it was inevitable that Sheldon would evaluate Lewis' finding in terms of the basic components of physique. Were the hebephrenics actually deficient in mesomorphy, or mesopenic? Gradually Sheldon anchored the old psychiatric terminology on a firm biological foundation by seeing that each one of three major psychiatric classifications could be looked at as the deficiency of one of the basic elements of physique. The hebephrenic schizophrenic lacked mesomorphy, the manic-depressive lacked ectomorphy, and the paranoid lacked endomorphy. Therefore, these newly created psychiatric poles would fall on the somatotype chart opposite the somatotype and temperamental poles.
With this hypothesis in hand, Sheldon noticed as he poured through hundreds of psychiatric records that the greatest variability in diagnosis centered on certain kinds of patients. The midrange somatotypes, as would be expected, were described in a variety of ways, but intriguingly the patients that fell at morphological poles, that is, midway between the psychiatric poles, were also given a greater variety of diagnoses than those that fell near the psychiatric poles.
Sheldon set out to test this insight in a more scientific manner. In 1945 he initiated an experiment with Phyllis Wittman at Elgin State Hospital in Illinois. Wittman created a checklist of psychotic behavior reactions, somewhat similar to Sheldon's checklist of temperament, but only this time the main components were affective-connative exaggeration, paranoid projection and schizoid regression. Each of these basic components was described by ten traits, and each of the traits was to be evaluated on a scale ranging from I to 7. With this checklist in hand it was soon demonstrated that two psychiatrists could reach a large measure of agreement in evaluating patients. In the meantime Sheldon had independently photographed and somatotyped 155 psychotic male patients. Then the psychiatric evaluations that Wittman had made from the psychiatric records and Sheldon's somatotype ratings were turned in independently for statistical analysis. The correlations were sufficiently high to lend good support to Sheldon's attempts at creating an integrated way of viewing psychiatric illness. The manic-depressive psychiatric component correlated +.54 with endomorphy, +.41 with mesomorphy and -.59 with ectomorphy. The paranoid component correlated -.04 with endomorphy, +.57 with mesomorphy and -.34 with ectomorphy, while the third or hebephrenic component correlated -.25 with endomorphy, -.68 with mesomorphy and +.64 with ectomorphy. These correlations would have even been higher if allowance had been made for the fact that the psychiatric poles were 600 away from the morphological poles.
In another experiment Sheldon correlated his psychiatric evaluation of the 155 patients by means of the somatotype performance test with Wittman's ratings taken from the psychiatric records. The performance task was simply how well the patient could hold the standard somatotype pose while the picture was being taken. If the hebephrenic component predominated, for example, the patient could not hold his arms in full extension, that is, as if he were standing at attention. Again, Sheldon was reading in the somatotype the psychiatric condition of the patient. The two evaluations correlated +.71 for the first component, +.76 for the second component and +.82 for the third component.
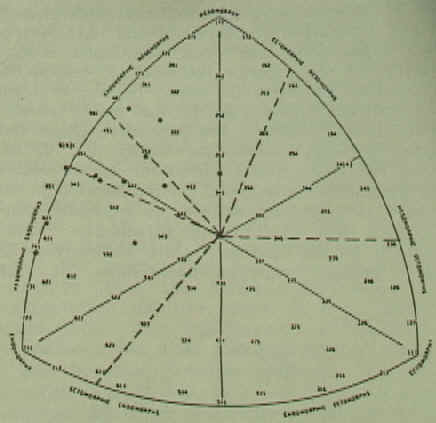
Fig. 9. Manic-Depressive Somatotypes
If we look at the somatotype charts on which Sheldon plotted the three major psychiatric divisions of these Elgin Hospital patients, we see that the cluster of manic depressive patients is much like Sheldon anticipated, for they are well grouped in opposition to the pole of ectomorphy. From the point of view of the relationship between psychological type and somatotype we would expect them to be extraverted with predominant sensation and thinking and sensation and feeling. This agrees fairly well with Van der Hoop's evaluation that the manic-depressive is an extraverted sensation type, but not with his impression that they are extraverted intuition types. It is also close to the extraverted feeling sensation type that Bisbee, Mullaly and Osmond found, but not to their extraverted intuition thinking type and the introverted feeling intuition type. It may well be that the extraverted sensation thinking type in a manic phase of behavior simulates well the quick changeability and innovative character of the extraverted intuition type. Jung was once questioned about the variability of the superior function and responded, "If you consider the case of manic depressive insanity, you occasionally find that in the manic phase one function prevails, and in the depressive phase another function prevails." (Collected Works, V. 18, p. 31) Keirsey and Bates state, "Sensation seems equivalent to Kretschmer's cyclothymic temperament." (p. 30)
There is a certain amount of evidence that the extraverted and cyclothymic personality traits are related to bipolar disorder, while introversion is related to primary non-polar depressions. (cf. Akiskal, "The Relationship of Personality to Affective Disorder") Unfortunately, attempts to distinguish the various kinds of affective diseases often do not take somatotype into account.
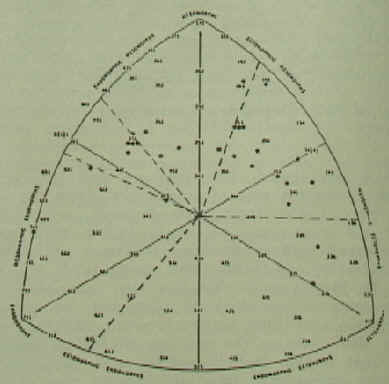
Fig. 10. Paranoid Schizophrenic Somatotypes
Sheldon's somatotype chart of the paranoid schizophrenics show the majority of patients
clustered in the area opposite the pole of endomorphy, as he anticipated. The paranoid
component showed a positive correlation with mesomorphy, but was virtually neutral in
regards to endomorphy, and instead of a positive correlation with ectomorphy it showed a
negative correlation (-.34). What could explain these unexpected correlations? If we are
correct in our evaluations of the psychological types connected with the somatotypes, then
the paranoid personalities cover the extraverted intuitive range. It is a fairly
well-established fact that the paranoid schizophrenics are more mesomorphic than the
hebephrenic schizophrenics, and they have a better prognosis. This has been demonstrated
from the point of view of Sheldon's somatotypes by Kiln and Tenney, and the difference in
body build between the two groups has also been demonstrated by means of the Rees-Eysenck
body index. From the psychological point of view it could well be that the more
extraverted paranoid schizophrenics share the same saving grace of many of the
manic-depressives in that their extraversion keeps them in touch with the outer world,
while the introverted hebephrenic schizophrenics lose contact. Does the extraversion of
many of the paranoid personalities mute the opposition that would be expected to the pole
of endomorphy because of the common extraversion involved? And at the same time, does this
extraversion accentuate the difference between the paranoid component and the pole of
ectomorphy which we are taking as an introverted pole?
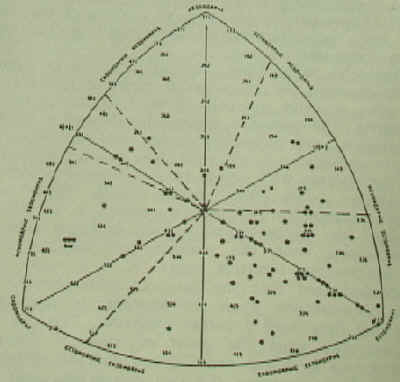
Fig. 11. Hebephrenic Schizophrenic Somatotypes
The final chart shows the hebephrenic schizophrenics grouped predominantly near the ectomorphic pole. Sheldon found that the third psychiatric component showed the expected correlation with ectomorphy (+.64) and the expected negative correlation with mesomorphy (-.68), but instead of a positive correlation with endomorphy there was a negative one (-.25). If the schizophrenics are lacking in mesomorphy, why do they cluster about the pole of ectomorphy rather than opposite the pole of mesomorphy? Sheldon suggests that in the particular sample he was working with the more mesopenic personalities could have already collapsed and literally could not stand up and have their picture taken. This would help explain the failure to find a positive correlation with the pole of endomorphy. Bisbee and her colleagues found a high number of introverted sensation types among the schizophrenic patients. This may be due to the fact that these patients were actually introverted sensation types which had already disappeared from Sheldon's sample, but here were caught at the beginning of their hospital stay, or it may be that the introverted intuitive types are more highly represented among schizophrenics and only appear like introverted sensation types and this would explain their clustering around the ectomorphic pole and their opposition to the pole of endomorphy. For Keirsey and Bates "what Jung called intuition appears to be equivalent to Kretschmer's schizothymic temperament". (p. 30) Once again, there are a number of cases in the 4-4-2 and 4-5-2 area that are found in the paranoid schizophrenic samples, and it is possible that these represent the introverted thinking sensing or introverted feeling sensing people who are classified as either schizophrenics or paranoids instead of manic-depressives.
Various aspects of Sheldon's psychiatric work have found independent confirmation. Parnell, for example, made extensive studies of the somatotypes and ages of the various categories of mental patients. He found that earliest admissions started around the ectomorphic pole of the somatotype chart, and then seemed to proceed counter-clockwise. The mesopenic ectomorphs broke down first, but at later ages, the more mesomorphic and endomorphic somatotypes ran into psychiatric difficulties. Parnell's somatotype chart of 22 consecutively admitted male schizophrenics shows roughly the same distribution as Sheldon's, with the highest incidence in what we have called the introverted intuitive territory. He also shows the paranoid schizophrenics as more mesomorphic than the other forms of schizophrenics, again with roughly the same kind of distribution as Sheldon's.
Sheldon's insights about the lack of mesodermal development in schizophrenics must be seen against the background of the various studies on the cardiovascular apparatus of schizophrenics. Some of them have been summarized by Arieti and show that the blood pressure of schizophrenics is lower than that of the general population with the highest values found in the paranoids and the lowest in the catatonics. The volume of circulating blood in schizophrenics has been found to be smaller than in manic depressives, and there is a tendency toward vaso-constriction, when schizophrenics are exposed to cold temperatures. Arieti summarizes the alterations under the headings of a "(1) decrease in the size of the heart; (2) decrease in the volume of the blood flow; (3) decrease in systematic blood pressure; (4) exaggerated tendency to vasoconstriction and resulting diminished blood supply." (Interpretation of Schizophrenia, p. 465) Additional studies have focused on the immature capillary structure of schizophrenics and the particular capillary pattern in their nail folds. It's easy to see here the dilemma that psychiatrists face when they attempt to interpret these findings without any awareness of the underlying normal variations of personality. What would happen if the blood pressure of the schizophrenics was compared not to the normal population, but to the introverted intuitive personality? Arieti also mentions that these kinds of studies tapered off after 1955. Why? The search for an answer can be informative, for it will allow us to breach the question of a biochemical typology from another direction.
We saw Sheldon, beset from within and without, losing heart with the 1949 publication of the Varieties of Delinquent Youth. This is especially regrettable because if he would have only used his Promethean foresight he might have sensed the first signs of a shift of psychological climate away from the prevailing environmentalism in psychiatry.
Off in Australia in obscurity that same year John Cade had begun experimenting with lithium, which was to lead to a new treatment of manic-depressives. In St. Louis in the 1950s men like Eli Robins, Samuel Guze and George Winokur were initiating a neo-Kraepelinian revival which wanted to strengthen the ties between psychiatry, medicine and neuroscience. In Paris, 1952, two French psychiatrists, Jean Delay and Pierre Deniker, were experimenting with chlorpromazine, which was going to have such a dramatic effect on the treatment of mental disease all over the world. In 1950 John Smythies and Humphrey Osmond had noticed that the molecular structure of mescaline was close to that of adrenaline, and they reasoned that a faulty metabolism in schizophrenics might alter the adrenaline and give it a psychedelic function. This led to the work of Hoffer and Osmond with niacin, and vitamin C in the treatment of schizophrenia, and became one of the sources of orthomolecular medicine, and it had another unexpected side-effect. Osmond, in the course of his experimentation, took mescaline in order to experience something similar to what his patients were undergoing. His first paper on the subject brought a letter from Aldous Huxley, and it was Osmond who helped send Huxley on his first mescaline trip which was to lead to Huxley's The Doors of Perception. In turn Huxley introduced him to Sheldon and his work in a novel way: "On one of our shopping expeditions in Orbachs, Los Angeles, Aldous introduced me to the art of escalator somatotyping. People on escalators are unselfconscious, unaware of scrutiny and at their ease. As we were wafted by them passing in the opposite direction, Aldous would call out, "Humphrey, did you see that marvelously somatotonic woman with the Aztec features?" Further, it was Huxley and Osmond who met and encouraged Timothy Leary to undertake serious psychotropic drug research in 1960, and thus, somewhat inadvertently, helped spark the psychedelic revolution in the United States.
In addition, one of Sheldon's former students, Nathan Kline, played an important role in the transition from a psychoanalytically oriented psychiatry to a more biological one. Almost accidentally he became involved in testing reserpine, a drug extracted from a plant that grows in the hill country of India and which had been used for ages in Indian folk medicine, and achieved good results by calming disturbed schizophrenics. Then he reasoned that if there was a chemical compound that would calm people, there should be another one that would excite them, and he found it in iproniazid, and it had a remarkable effect on people suffering from severe depression. This work had coincided with the discovery in Switzerland of imipramine, the first of the important tri-cyclic anti-depressants.
In his 1957 review of Sheldon and Eleanor Glueck's Physique and Delinquency Sheldon amplifies some of his remarks that appeared in Varieties of Delinquent Youth on how to view somatotypes: "They are aware that the somatotypic description of an individual, far from supplying an explanation of all his conduct, is actually no more than a necessary starting point, or organizing principle, from which to initiate a study of conduct and behavior." (p. 125) Then he quotes Kline and Tenney whom the Gluecks had quoted, as well:
"The ultimate answers probably lie in the biochemical and biophysical fields. Direct approach to the problem through biochemistry and biophysics has, however, resulted in a welter of data that are consistent only in the fact that they are extremely variable. We have already obtained considerable information-which leads us to believe that many physiological responses - and ultimately the biochemical and biophysical relations upon which they rest - vary in direct relationship with somatotype. The introduction of somatotyping as an 'organizing principle' may quite possibly make order out of what is now chaos because of individual differences." (N.S. Kline and A.M. Tenney, "Constitutional Factors in the Prognosis of Schizophrenia", p. 441.)
But like a biologically oriented Moses Sheldon saw the promised land, but never entered it. And this new psychiatry has been so preoccupied with its fascinating discoveries it has not yet had time to remember the work of the typologists, although they inevitably have to face typological issues. Rosenthal and his colleagues, for example, in an evaluation of the children of schizophrenics reared in adoptive homes, found data that suggests: "that the inherited core diathesis is the same for both schizophrenia and manic-depressive psychosis, but that manic-depressives may have other modifying genes or life experiences which direct the clinical manifestations of the diathesis in a different way." (1968, p. 387) The same causative agent might very well appear differently and show itself as hebephrenic schizophrenia in one instance, paranoid schizophrenia in another, or even manic-depression in a third.
There really is no normal or average personality. The evidence seems clear that certain kinds of individuals are more prone to schizophrenia or one of the other major illnesses than others. But we have really yet to fully utilize this kind of information. We are faced with an embarrassment of riches. We have innumerable studies which are tremendously hard to bring together within a common framework, and one of the elements of that common framework is a common way of describing the normal personality at the level of somatotype, temperament and psychological type. If we could understand the biochemistry and genetics of the normal personality we could take this knowledge into account when we study the psychiatric patient. Instead, we are studying both the illness and the distinctive structure of the normal personality at the same time. Whatever the particular metabolic dysfunction schizophrenia turns out to be, it is a dysfunction that is going to effect each particular type in a particular way. We differ in our susceptibility, in symptomotology, and prognosis because we differ normally in the very chemistry of our brains.